Invisalign® clear aligner technology is growing in the number of patients treated annually. According to the Align Technology Annual Report, the statistics regarding patient adoption rates worldwide now show over 4 million patients have used Invisalign technology to straighten their teeth. Orthodontists should wisely consider this growing marketplace as an area to expand their practices to take advantage of the immense opportunities, especially as the market becomes ever more competitive.
Your orthodontic practices can greatly benefit from expansion into the Invisalign marketplace. Opening the door for more opportunities to serve the adult and teen market makes it a terrific way to grow your practice.
To do this, you will need education about the latest Invisalign treatment techniques. This knowledge will help you understand Invisalign’s potential value through the technology’s capabilities. It may even inspire you to broaden your orthodontic patient solutions, practices, and methodologies to achieve winning results.
There are many ways to learn more about treating patients with Invisalign clear aligners, including webinars and lectures archived on the Invisalign Doctor Site, as well as live clinical education events. Despite these resources, many doctors still tell me they hesitate to treat more of their patients with Invisalign clear aligners because they don’t understand how to interpret what they see on their 3D ClinCheck® virtual treatment plans, nor do they understand when and where ClinCheck plan modifications are required. What many doctors who are inexperienced at treating patients with Invisalign really need is a personal coach—an Invisalign expert who can guide them through the ClinCheck treatment planning process on a personalized, one-on-one basis. This is exactly what AlignerInsider.com offers. After registering for a membership, you get access to a video library of expert aligner training resources and a walk-through for various Invisalign-based cases as well as educational and professional videos on marketing for your practice.
Inside the Book
Orthodontic Products talks to Barry J. Glaser, DMD, about his new book The Insider’s Guide to Invisalign® Treatment, which will be released in the spring.
OP: What prompted you to write this book?
Glaser: When I set out to write The Insider’s Guide to Invisalign® Treatment, my objective was to develop a user-friendly, systematic guide to virtual treatment planning with Invisalign. Throughout my travels lecturing to doctors about treating patients orthodontically with Invisalign, a common theme I hear is that many doctors don’t “get” Invisalign, meaning they don’t understand how to interpret what they see on a ClinCheck® treatment plan, nor do they understand how to effectively communicate their treatment goals to their technician.
Designed for both the novice as well as the more experienced user, the book features a 10-step systematic guide to virtual ClinCheck treatment planning I call the “ClinCheck List.” Using a wide variety of patients I have successfully treated with Invisalign clear aligners, the book takes the reader through a rational, common sense, step-by-step approach to Invisalign treatment planning. In addition, the reader will learn my many tips and tricks for more efficient treatment as well as trouble-shooting for common problems encountered during clear aligner treatment.
OP: What can the Invisalign skeptic, and the Invisalign expert, learn from this book?
Glaser: I think the skeptic will be surprised to see that excellent results can be achieved predictably with Invisalign treatment even in quite complex malocclusions. Furthermore, the book will demystify the virtual treatment planning process so that they too can achieve consistently excellent results in their own Invisalign cases.
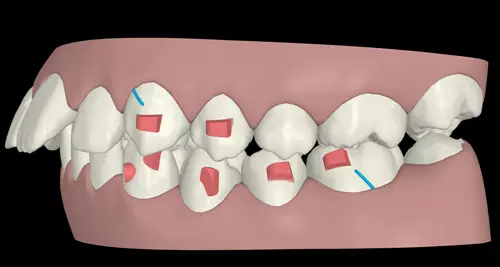
For the Invisalign expert, I think my unique way of viewing a ClinCheck animation as a depiction of the forces acting upon the teeth rather than a prediction of the final occlusion will help them view their own ClinCheck plans in a completely novel and enlightening way, and will help them treat their own patients in a more efficient and predictable manner.
OP: You were once an Invisalign skeptic. What changed your view about Invisalign?
Glaser: I was a huge skeptic! But I also recognized that as a practitioner, it was critically important to the success of my practice that I continue to embrace the rapidly changing nature of our profession. To keep up with changing trends, as well as the demands of my own 21st century patients—including teens—or more aesthetic and convenient treatment techniques, it was necessary to offer Invisalign as a treatment option. I quickly realized that if I wanted to offer the very best service to my patients, I had to educate myself. So, I began attending every live Invisalign educational event I could, read all the articles I could get my hands on, and viewed all the educational webinars offered on my Invisalign Doctor Site. Before long, I found myself up at the podium teaching other doctors about excellence in orthodontics with Invisalign.
OP: Besides yourorthocoach.com, what other Invisalign education efforts have you been involved with?
Glaser: Doctors have yet another avenue for Invisalign education right from their computer. I founded AlignerInsider.com as the premier resource for education in excellence with aligner orthodontics. Version 2.0, soon to be released, represents a major upgrade to the original site. In partnership with Willy Dayan, DDS, treatment coordinator and consultant Laura Cafik-Martin, and marketing expert Dean Steinman of OrthoMarketing.com, alignerinsider.com is a rich resource for further Invisalign education. Featuring a phenomenal library of exclusive educational videos for both doctors and staff that may be viewed 24 hours a day, alignerinsider.com not only helps doctors and their practices achieve better and more efficient results with Invisalign treatment, but it also provides expert marketing tips and staff training. Soon to be released enhancements include exclusive live webinars as well as a “social media” component where doctors and staff around the world will be able to interact online to discuss aligner-related topics.
OP: What do you hope to accomplish with your involvement with these two online-based services?
Glaser: I highly recommend the book, The 4 Hour Work Week by Tim Ferriss. I am passionate about teaching; however, the demands of my practice and family prevent me from travelling to teach as much as I would like. Virtual, computer-based education via alignerinsider.com and yourorthocoach.com allows me to adopt a “4 Hour Work Week” model, reaching a large audience of doctors literally around the world without ever leaving my home town.
As an Align Faculty member, I travel the world teaching doctors about achieving excellence with Invisalign clear aligners for both their adult as well as teen patients. My inbox was flooded with emails from doctors and Invisalign reps looking for individual help with their Invisalign cases. When Dayan approached and asked me to join his team of coaches, I did not hesitate to accept. I immediately recognized this new paradigm of virtual coaching as “technology at its best.” For the first time, I could coach doctors anywhere in the world in a meaningful way from the convenience of my laptop computer.
Using my principles of ClinCheck design, I teach doctors to look at ClinCheck not as a prediction of the final occlusion, but rather as a visual representation of the forces being applied to the teeth by the aligners. Force systems, not teeth. These principles of systematic, common sense ClinCheck treatment planning are featured in my soon-to-be released textbook, The Insider’s Guide to Invisalign® Treatment.
Twenty-first century technology has opened up an exciting arena for computer-based orthodontic education. As computer-assisted orthodontic technologies such as Invisalign clear aligners continue to grow in the orthodontic marketplace, educational opportunities have emerged to capitalize on the virtual treatment planning tools offered via the ClinCheck software. Doctors now have at their disposal the ability to call upon a virtual mentor to personally guide them in the treatment planning process for their Invisalign cases. The educational video lessons from the coaches at yourorthocoach.com are viewable 24 hours a day from your desktop computer, laptop, or mobile device, whether at the office, at home, or on the go. Clinical confidence treating a wider variety of malocclusions with Invisalign clear aligners develops quickly, while treatment outcomes become more predictable and efficient. Ultimately, the doctor as well as the patient benefit. I encourage you to take advantage of this incredible technology to help keep up with rapidly changing trends in orthodontics.